1. What is a Multi-Disciplinary Team meeting?
Multi-disciplinary team (MDT) meetings are often held in order to coordinate health and care services to meet the needs of individuals with complex care needs. A MDT meeting may be convened with professionals across one or more disciplines within an individual organisation, however appropriate consideration must always be given to including all relevant professionals involved in the care and support of the involved adult, to ensure a consistent, co-ordinated and person-centred approach to their care.
2. What is the purpose of this guidance?
As stated above multi-disciplinary team (MDT) meetings are often held in health and social care settings; however, the principles of a good MDT meeting can be applied to many other areas of work. This is a practical guide to help individuals, teams, managers, and agencies when arranging and/or attending meetings which focus on integrated working, improving outcomes for individuals and improving communications.
3. Why hold a Multi-Disciplinary Team meeting?
A good MDT meeting will:
- clearly identify roles and responsibilities
- remove duplication and avoid repetition
- ensure good documentation that supports a way of working in a more productive way
- will improve the experience for staff by:
- reducing repetition of information recording and transfer
- maximising the time for direct work
- improving documentation by making it easier to access and to understand what is happening
- reduce the number of meetings that you attend or call unnecessarily
- improve the quality of the outcomes that you achieve in your meetings
- improve the responsiveness to actions being followed up by participants
- improve the quality of the preparation that is undertaken
- improve the quality of conversations
- improve the level of participation
- improve multi-agency working relationships / networks and peer support
- improve liaison with partners, particularly health colleagues, to support proactive planning and coordination. Where relevant, MDTs should consider whether individuals are included on the Dynamic Support Register (DSR), ensuring this information is appropriately reflected in care planning.
- involve individuals, carers and families in discussions to ensure that their views and interests are central to the decision making
- identify a key worker through which care and support is coordinated by a named team member. The key worker should be a practitioner who is acceptable to the individual and knows them best
4. Learning from Practice
Case Study: NB (Age 41)
NB had a history of trauma, domestic abuse, substance misuse, and periods of deteriorating mental health, including suicidal thoughts. NB had been referred into the National Referral Mechanism (NRM) with a reasonable grounds decision made. Despite multiple agencies being involved, MDT meetings were delayed and sporadic. A transfer of care between teams lacked a formal handover, leaving NB without social work support for weeks. Missed appointments and closed referrals occurred because agencies didn’t share updates. NB was assessed as at risk of death, but coordination and escalation were insufficient. NB died in October 2024 from drug misuse.
Key Learning:
- Early and consistent MDT coordination: Delays in convening MDT meetings and sporadic attendance led to fragmented care. Emails alone were insufficient for complex cases.
- Where multiple agencies are involved and significant risk is identified, an MDT meeting must be convened promptly. Email exchanges alone are not sufficient for complex cases.
- Lead Agency Identification – It was unclear who was leading NB’s care, which caused confusion and gaps in responsibility.
- At the first MDT meeting, agree and record the lead agency and named coordinator. This should be documented and shared with all partners.
- Formal handover during transfer of care – A 3-week delay and poor communication during transfer between teams left NB without social work support
- When transferring between teams, a formal handover meeting should occur, with outstanding actions documented and contact details shared with all agencies.
- Communication failures across agencies – Missed appointments and closed referrals occurred because agencies didn’t share updates or check reasons before closing cases.
- Before closing referrals, agencies must check with other MDT members to confirm reasons and avoid unintended gaps in care.
- Active case management for high-risk individuals – NB was assessed as at risk of death by misadventure, but coordination and escalation were insufficient.
- If a person is assessed as at risk of serious harm or death, escalate immediately to senior managers and consider increased MDT frequency, maintain proactive communication and joint planning to discuss individual agency concerns and agree a plan of action for roles and responsibilities. In addition, review whether a referral to safeguarding is required and where other multi-agency processes have not been successful in reducing risk or harm and where a strategic approach to case oversight is required, explore other risk management forums such as the High-Risk Adults Panel (HRAP).
5. What should be considered when setting up a Multi-Disciplinary Team meeting?
The following questions should be considered:
- Does a meeting need to be held at all?
- What are the objectives of the meeting?
- Who needs to attend in order to achieve these objectives?
- What is known about the participants and what level of formality is required?
- Who will be the named key worker?
Key Principles to consider:
- Person-centred and outcome-focused planning
- Timely and coordinated multi-agency involvement
- Clear roles, responsibilities and accountability
- Professional curiosity and respectful challenge
- Robust documentation and information sharing
- Inclusion of individuals, carers and advocates
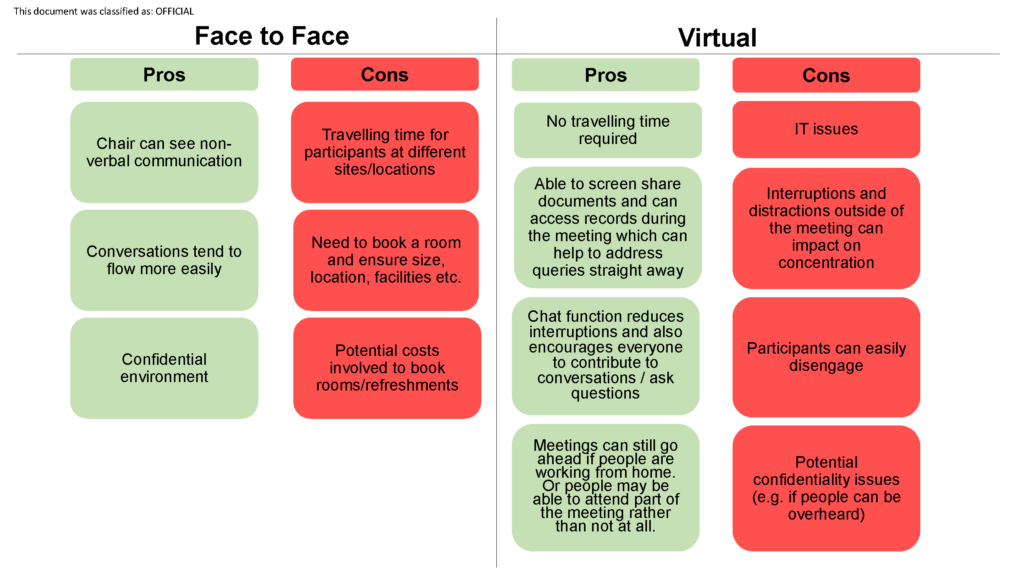
Once the above have been considered, the format of the meeting should be agreed. This may be a face-to-face meeting or a virtual meeting (e.g., using Microsoft Teams or Zoom). There are pros and cons which should be weighed up:
6. Preparing for a Multi-Disciplinary Team meeting
- Identify the Chairperson and ask for their availability
- Identify others who should be invited to cover the meeting objectives and ask for their availability
- Identify a named key worker
- Check availability of appropriate meeting rooms (for face-to-face meetings)
- Schedule the meeting for a time (and place) that is convenient for all and send calendar invitations
- Book the venue and any equipment or facilities needed (for face-to-face meetings)
- Ensure all participants have suitable IT access (for virtual meetings)
- Ensure all the relevant professionals/agencies are represented
- Agree the agenda
- Assign a note taker to capture minutes and actions
- Send out the agenda in advance of the meeting with clearly stated objectives
7. Information Sharing
It will be necessary to consider how information will be shared, particularly where personal information is involved. There may already be an Information Sharing Agreement in place, for example in relation to Safeguarding Adults, however, this may not always be the case and can become a barrier to ensuring an effective meeting is held. It is important that advice is sought from Information Governance to address any issues that may arise in relation to information sharing.
8. Attending a Multi-Disciplinary Team meeting
- Prepare adequately for the meeting:
- read the agenda and papers
- consult the individual/family/carer on their views, wishes and interests
- complete any actions and be prepared to provide an update.
- The Chairperson should set and agree the ground rules, which may include:
- start and finish the meeting on time
- minimise any disturbance and/or interruptions
- ensure the ‘day job’ is covered
- ensure an appropriate deputy is available to cover any periods of absence and is appropriately briefed
- ensure that the meeting is confidential and cannot be overheard by others (e.g., if people are working from home).
- Participate in the meeting:
- be prepared to be professionally curious and to challenge participants – see TSAB’s Professional Curiosity Guidance
- provide all relevant information and updates to the meeting
- listen to what others have to say
- stay on track with conversations
- seek clarification if unsure
- be open to other participant’s opinions
- try not to be negative
- try not to ‘take over’ the meeting
- be prepared to take away actions from the meeting, if you feel these are unrealistic or not achievable, say so.
- Follow up:
- Take ownership of any actions allocated to you and complete as promptly as possible
- Pass on relevant information within your team/ organisation
- Key worker to provide feedback, actions and options from the meeting to the individual/family/carer
9. Record Keeping
Robust records of any MDT meeting should be taken and stored for future reference in line with the Information Sharing Agreement and/or the hosting organisation’s Document Retention Policy.
It is important to record who was present and which team/organisation they represent: this will help to identify if a team or organisation is not represented and perhaps should be. It will also be a useful record to evidence persistent non-attenders.
Agree and record the lead agency and named coordinator, this should be shared with all partners.
Sufficient detail should be recorded in the minutes to record the discussion points and any actions identified and who is responsible for these actions including timescales. The minutes should be circulated to all who attended the meeting and you should consider sending to those who were invited but were unable to attend.
10. Summary; Effective Meeting Tips
- know why you are there
- be there on time
- agree and record the lead agency and named coordinator, and share this with all partners
- stay on the subject
- be respectful to the chairperson and other participants
- be open to the ideas of others
- help the chairperson control the meeting
- share best practice
- engage individuals and families in discussions and decision making.
- Before closing referrals, check with other MDT members to confirm reasons
Version Control:
February 2026 – Version 3